


Annual Cost Paid With 12 Month Agreement
Single Enrollee
Enrollee + 1 Family Member
Each Additional Family Member
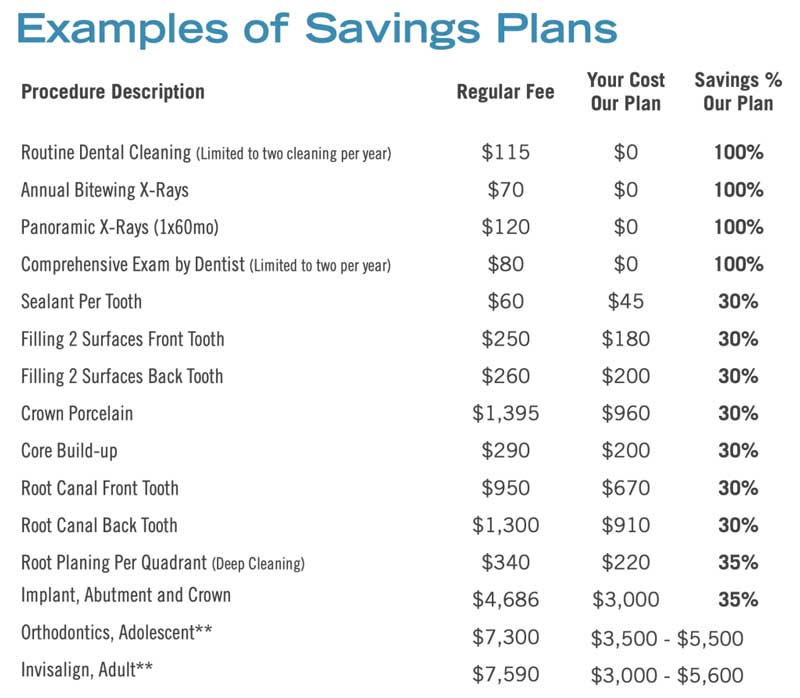
Examples of Savings Plans
| Procedure Description | Regular Fee |
Your Cost Our Plan |
Savings % Our Plan |
|---|---|---|---|
| Routine Dental Cleaning (Limited to two cleaning per year) | $145 | $0 | 100% |
| Annual Bitewing X-Rays | $90 | $0 | 100% |
| Panoramic X-Rays (1x6mo) | $151 | $0 | 100% |
| Comprehensive Exam by Dentist (Limited to two per year) | $114 | $0 | 100% |
| Sealant Per Tooth | $76 | $47 | 35% |
| Filling 2 Surfaces Front Tooth | $314 | $189 | 35% |
| Filling 2 Surfaces Back Tooth | $327 | $210 | 35% |
| Crown Porcelain | $1,743 | $1,008 | 35% |
| Core Build-up | $365 | $210 | 35% |
| Root Canal Front Tooth | $1,188 | $703 | 35% |
| Root Canal Back Tooth | $1,625 | $955 | 35% |
| Root Planing Per Quadrant (Deep Cleaning) | $426 | $231 | 35% |
| Implant, Abutment and Crown | $6,257 | $3,150 | 35% |
| Orthodontics, Adolescent | $9,077 | $4,000-$6,000 | |
| Invisalign, Adult | $9,077 | $5,000-$6,000 |
Terms and Conditions
I am applying to enroll in the Our Plan dental plan program with Boulder Dental Services for a minimum of one year. I will remain on the plan and pay membership fees for a minimum of 12 months. There is not cancellation or termination option for the annual period agreed upon. Fee’s for dental services provided at the discounted rate are due at the time of service. Fees for restoration and prosthodontic services are due at the preparation and impression visit. Failure to provide payment at time of service may result in being charged usual and customary fees. Renewal of plan will occur automatically at your annual renewal date unless otherwise notified by you.
By agreeing to these terms and conditions, I affirm that I understand the payment conditions and dental services provided under this plan. Pursuant to the Health Insurance Portability and Accountability Act of 1996, my acceptance authorizes the Boulder Dental Services organization to utilize my Protected Health Information (PHI) to carry out treatment, payment and healthcare operations. I understand that it is the policy for Boulder Dental Services to only utilize the minimum PHI to facilitate my treatment under this plan.
Dental Limitations and Exclusions
The plan only includes services as outlined in the complete fee schedule. Patient will only receive services when deemed clinically necessary by practicing dentist or dental hygienist. Plan does not include medications provided at the dental office, general anesthesia, any services requiring the involvement of a non-participating specialist, orthodontic services or any procedure not performed by participating dentist. Furthermore, this plan does not cover any dental procedures performed outside a Boulder Dental Services office locations.